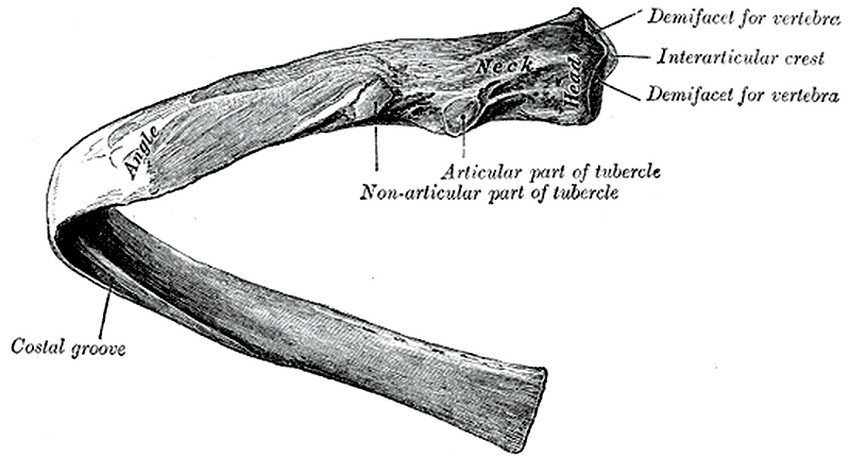
Thoracic rib, Posteroinferior view
The ribs form the lateral bony wall of the thorax. The ribs are paired and there are 12 pairs of ribs in the human thorax, most of them connecting the thoracic spine with the sternum. They are numbered from superior to inferior.
Ribs have different anatomical characteristics depending on their level. A typical rib has the following characteristics from posterior to anterior:
• Head: The head of each rib articulates with one or two ribs depending on their level. Typically ribs number 1,2, 10, 11, and 12 articulate with one vertebra, while the rest articulate with two vertebrae.
• Facets: These are the articular surfaces found in the head of each rib. They are covered by hyaline cartilage and form part of the costovertebral synovial joints. In the case of ribs 3 to 9, since they articulate with two vertebrae, they have two facets, each one called a demifacet, with an interarticular crest between them.
• Neck: A short, somewhat narrower portion of the rib that projects straight posterolaterally.
• Costal tubercle: A bony protuberance, usually with two components, one articular and one non-articular. The articular part of the costal tubercle presents with a facet that articulates with the transverse process of a thoracic vertebra.
• Costal angle: A sharp posterior curvature of the rib. The body when supine rests of these costal angles which deflect pressure from the thoracic spine.
• Costal body: The area of the rib anterior to the costal angle. In most ribs this oval-shaped region of the rib presents with an inferior and internal groove. This is the costal groove or costal sulcus. The corresponding level intercostal artery, vein, and nerve are found in the costal sulcus.
• Costal cartilage: All ribs have an anterior fibrocartilaginous component. Some of them attach directly to the sternum (chondrosternal joints), while some of them attach only to other costal cartilages (chondrochondral joints).
The 12 pairs of ribs are divided as follows:
• True ribs: Ribs 1-7, which attach by way of their costal cartilage directly to the sternum
• False ribs: Ribs 8-10, whose costal cartilage attach only to the cartilage of the superior rib, creating a lower border for the thoracic cage known as the costal margin.
• Free or "floating" ribs: Ribs 11 and 12. Their anterior cartilaginous end does not attach to sternum or other cartilage, so the end is free. The term "floating" although used, is a misnomer as these ribs do attach posteriorly to the thoracic spine.
There can be anatomical variations to the ribs, including the existence of extra cervical or lumbar ribs.
Sources:
1 "Tratado de Anatomia Humana" Testut et Latarjet 8 Ed. 1931 Salvat Editores, Spain
2. "Anatomy of the Human Body" Henry Gray 1918. Philadelphia: Lea & Febiger
Original image courtesy of bartleby.com. For more information: click here

{kind=link}