![]()
Medical Terminology Daily (MTD) is a blog sponsored by Clinical Anatomy Associates, Inc. as a service to the medical community. We post anatomical, medical or surgical terms, their meaning and usage, as well as biographical notes on anatomists, surgeons, and researchers through the ages. Be warned that some of the images used depict human anatomical specimens.
You are welcome to submit questions and suggestions using our "Contact Us" form. The information on this blog follows the terms on our "Privacy and Security Statement" and cannot be construed as medical guidance or instructions for treatment.
We have 1260 guests online
")
Marcia Crocker Noyes
(1869 – 1946)
Further to my comment on old books and research that started with an interesting bookplate (Ex-Libris). I continued my research and found that the person in charge of the Osler library bookplate was a fascinating individual that today maybe a ghost in the MedChi library and building in Baltimore... This is certainly an article that can be called "A Moment in History"
Marcia Crocker Noyes was the librarian at The Maryland State Medical Society from 1896 to 1946 and was a founding member of the Medical Library Association.[1][2][3]
Sir William Osler, MD. a famous Johns Hopkins surgeon was a noted bibliophile and had a large personal collection of books on various topics. When he became the President of MedChi in 1896, he was dismayed at the condition of the library and knew that with the right person and some stewardship, it could become a significant collection. Sir William asked his friend, Dr. Bernard Steiner, a physician and President of the Enoch Pratt Free Library in Baltimore for suggestions of a librarian, and Dr. Steiner recommended Marcia Crocker Noyes. A native of New York, and a graduate of Hunter College, Marcia had moved to Baltimore for a lengthy visit with her sister, and took a “temporary” position at the Pratt Library, which turned into three years. Although she had no medical experience or background, she was enthusiastic, and most importantly, she was willing to move into the apartment provided for the librarian, who needed to be available 24 hours a day.
The image in this article is Ms. Noyes on her first year on the job. Marcia developed a book classification system for medical books, based on the Index Medicus, and called it the Classification for Medical Literature. The system uses the alphabet with capital letters for the major divisions of medicine and lower-case ones for the sub-sections. The system was used for many years, but it's now dated and the Faculty's original shelving scheme was never changed. The card catalogs still reflect her classification and many of the cards are written in Marcia's back-slanting handwriting.
Marcia knew enough to ask the Faculty's members about medical questions, terminology and literature. She gradually won over the predominantly male membership and they became her greatest allies; Sir William at the start, and then for nearly 40 years, Dr. John Ruhräh, a wealthy pediatrician with no immediate family of his own. She made a point of attending almost every Faculty function, and in 1904, under guidelines from the American Medical Association, Marcia was made the Faculty Secretary. For much of her first 10 years, she was the Faculty's only full-time employee, only being assisted by Mr. Caution, the Faculty's janitor. Later in life Marcia would say that she hired him because of his name!
Within ten years, the library had outgrown its space, and plans, spearheaded by Marcia and Sir William before his move to Oxford, were made to build a headquarters building, mainly to house the library's growing collection of medical books and journals.
Marcia was instrumental in the design and building of the new headquarters. She travelled to Philadelphia, New York and Boston to look at their medical society buildings, and eventually, the Philadelphia architectural firm, Ellicott & Emmart was selected to design and build the new Faculty building. Every detail of the building held her imprimatur, from the graceful staircase, to the light-filled reading room, and all of the myriad details of the millwork, marble tesserae, and most of all, the four-story cast iron stacks. She was on-site, climbing up unfinished staircases, checking out the progress of the building, which was built in less than one year at a cost of $90,000.
Among the features of the new building was a fourth-floor apartment for her. She referred to it as the "first penthouse in Baltimore" and it had a garden and rooftop terrace. The library collection eventually grew to more than 65,000 volumes from medical and specialty societies around the world. Journals were traded back and forth, and physicians eagerly anticipated the arrival of each new issue. At the same time, Marcia was involved in the Medical Library Association as one of eight founding members. The MLA promotes medical libraries and the exchange of information. One of the earliest mandates of the MLA was the Exchange, a distribution and trade service for those who had duplicates or little-used books in their collections. Initially, the Exchange was run out of the Philadelphia medical society, but in 1900 it was moved to Baltimore and Marcia oversaw it. Several hundred periodicals and journals were received and sent each month, a huge amount of work for a tiny staff. In 1904, the Faculty had run out of room to manage the Exchange, so it was moved to the Medical Society of the Kings County (Brooklyn). But without Marcia's excellent administrative skills, it floundered and in 1908, the MLA asked Marcia to take charge once again.
In 1909, when the new Faculty building opened, there was enough room to run the Exchange and with the help of MLA Treasurer, noted bibliophile and close friend, Dr. John Ruhräh, it once again became successful. Additionally, Marcia and Dr. Ruhräh combined forces to revive the MLA's bulletin, which had all but ceased publication in 1908, taking the Exchange with it. This duo maintained editorial control from 1911 until 1926. In 1934, around the time of Dr. Ruhräh's death, Marcia became the first “unmedicated” professional to head the MLA. During her tenure, the MLA incorporated, the first seal was adopted, and the annual meeting was held in Baltimore. Marcia wanted to write the history of the MLA once she retired from full-time work at the Faculty, but her health was beginning to fail. She had back problems and had suffered a serious burn on her shoulder as a young woman, possibly from her time running a summer camp, Camp Seyon, for young ladies in the Adirondack Mountains. In 1946, a celebration was planned to honor Marcia's 50 years at the Faculty. But she was adamant that the physicians wait until November, the actual date of her 50 years. However, they knew she was gravely ill, and might not make it until then, so a huge party was held in April. More than 250 physicians attended the celebration, but the ones she was closest to in the early years, were long gone. She was presented with a suitcase, a sum of money to use for travelling, and her favorite painting of Dr. John Philip Smith, a founder of the Medical College in Winchester, Virginia. It was painted by Edward Caledon Smith, a Virginia painter who had been a student of the painter Thomas Sully.[4] She adored this painting and vowed, jokingly, to take it with her wherever she went.
The painting was not to stay with her for very long, for she died in November 1946, and left it to the Faculty in her will. Her funeral was held in the Faculty's Osler Hall, named for her dear friend. More than 60 physicians served as her pallbearers, and she was buried at Baltimore's Green Mount Cemetery. In 1948, the MLA decided to establish an award in the name of Marcia Crocker Noyes. It was for outstanding achievement in medical library field and was to be awarded every two years, or when a truly worthy candidate was submitted. In 2014, the Faculty began giving a bouquet of flowers to the winner of the award in Marcia's name, and in honor of her work. Much evidence exists for this tradition, as we know that the physicians, especially Drs. Osler and Ruhräh, frequently gave her bouquets of flowers. Marcia also cultivated flower gardens at the Faculty and decorated the rooms with her work.
Today, the MedChi building is open for tours and if the rumors are to be believed Ms. Marcia Crocker Noyes is still at work in her beloved library as the "resident ghost" [1][5]

NOTE: This article has been modified from the original Wikipedia article on Marcia Crocker Noyes. The article itself is well-written with interesting images of the subject. I would encourage you to visit it. The second insert is from book 00736 in my personal library and shows in pencil, the incredibly small handwriting of Marsha C. Noyes.
Sources:
1. "Marcia, Marcia, Marcia" MedChi Archives blog.
2. "Marcia C. Noyes, Medical Librarian" (PDF). Bulletin of the Medical Library Association. 35 (1): 108–109. 1947. PMC 194645
3. Smith, Bernie Todd (1974). "Marcia Crocker Noyes, Medical Librarian: The Shaping of a Career" (PDF). Bulletin of the Medical Library Association. 62 (3): 314–324. PMC 198800Freely accessible. PMID 4619344.
4. Edward Caledon BRUCE (1825-1901)"
5. Behind the scenes tour MedChiBuilding
"Clinical Anatomy Associates, Inc., and the contributors of "Medical Terminology Daily" wish to thank all individuals who donate their bodies and tissues for the advancement of education and research”.
Click here for more information
- Details
- Hits: 7646
This is the first article ever published in this blog, The original date was October 31st 2012. Since then, over one thousand articles have been published.
The term "bariatric" is a compound word with two Greek roots: [βάρος] (város), meaning "weight" or "pressure", and [γιατρός](giatrós) meaning "doctor, physician, or healer". The adjectival suffix [-ic] means "pertaining to". The term bariatric means "pertaining to weight-related medicine".
Bariatric surgery is on the rise. In the USA, the Center for Disease Control (CDC) has accumulated data on obesity since 1985, and has a dedicated area in their website on the topic. The most common bariatric surgery as of 2023-24 is the sleeve gastrectomy, where preservation of the stomach magenstrasse and the incisura angularis is extremely important.
The following animated image is based on the CDC information on obesity trends page and the increase in obesity between the years 1985 until 2010. If you click on this image you will download a PowerPoint presentation with these maps
 After 2010 the CDC changed the way they collect and publish yearly trends on Adult Obesity Prevalence, adding information on education, age, race, and ethnicity. The following image is this compound map for 2023. For additional information on obesity by the CDC click here.
After 2010 the CDC changed the way they collect and publish yearly trends on Adult Obesity Prevalence, adding information on education, age, race, and ethnicity. The following image is this compound map for 2023. For additional information on obesity by the CDC click here.
 The CDC has an Adult Body Mass Index (BMI) Calculator you can use here. If needed, the CDC also has a BMI Calculator for Children and Teens between the ages of 2 to 19 years of age.
The CDC has an Adult Body Mass Index (BMI) Calculator you can use here. If needed, the CDC also has a BMI Calculator for Children and Teens between the ages of 2 to 19 years of age.
Note: Google Translate includes an icon that will allow you to hear the pronunciation of the word
"Gastrointestinal Clinical Anatomy" and "Bariatric Surgery" are among the many educational topics offered by Clinical Anatomy Associates, Inc. Click here to see additional educational materials and lecture topics specifically designed for medical industry professionals.
- Details
This article is part of the series "A Moment in History" where we honor those who have contributed to the growth of medical knowledge in the areas of anatomy, medicine, surgery, and medical research.

Jean-Annet Bogros (1786 - 1825) French physician, surgeon and anatomist. He was born in Bogros, a village in the mountains d’Auvergne, France.His family wanted him to become a priest, but his inclination towards medicine took him to an apprenticeship in the Hôtel-Dieu de Clermont, a hospital under the tutelage of Drs. Fleury, Lavort, and Bertrand. He continued his studies in Paris where he excelled at anatomy. He soon became an intern in Paris Hospitals, and in 1817 he became an assistant at the Faculty of Medicine. He was praised for his anatomical and surgical skills.
In August 29, 1823 he submitted his thesis for his Doctorate in Medicine “Essai Sur L’Anatomie Chirurgicale de la Region Iliaque: Et Description D’un Nouveau Procédure Pour Faire La Ligature Arteres Epigastrique Et Iliaque Externe”. His thesis challenged and improved the technique of ligation of the epigastric and iliac vessels proposed by Abernathy and Astley Cooper. His teaching rivaled the Astley Cooper technique, with an emphasis on hemostasis that was well recognized at the time.
Today his name is eponymically tied to the subinguinal space of Bogros, a triangular area posterior to the superior pubic ramus, lateral to the space of Retzius. This area is bound anteriorly by the deep preperitoneal fascia, and posteriorly by the peritoneum. The medial boundary of this space is either the lateral wall of the urinary bladder, or a sagittal plane passing at the origin of the inferior (deep) epigastric vessels. The superior boundary is the inguinal ligament, while the inferior and lateral boundaries are not described.
Bogros died in 1825 when he was 39 years of age. His cause of death in unknown, but many postulate tuberculosis.
Unfortunately, he was a good and simple man and was described as being meek and soft-spoken. Because of this, he only left one posthumous publication (1827) “Mémoire sur la Structure des Nerfs” where he explains a novel system to inject and identify nerves. This publication, in French, can be read and downloaded here.
Some biographical articles wrongly show his name as Jean-Antoine Bogros, others change the name to Annet Jean Bogros. Both are not correct. In our research we could not find a portrait of Bogros, so we used the cover or his posthumous memoir on the structure of the nerves.
Sources:
1. “Totally Extraperitoneal Herniorrhaphy (TEP): Lessons Learned from Anatomical Observations” Xue-Lu Zhou; Jian-Hua Luo; Hai Huang, et al. Minimally Invasive Surgery 2021(1):5524986
2. "Crucial steps in the evolution of the preperitoneal approaches to the groin: An historical review" R.C. Read Hernia 2010. 15(1):1-5
3. "Retzius and Bogros Spaces: A Prospective Laparoscopic Study and Current Perspectives" Ansari, MM Annals of International Medical and Dental Research, 2017 Vol (3), Issue (5) 25-31
4. " The Preperitoneal Space in Hernia Repair" Lorenz, A et al. Front Surg (2022) Visceral Surgery Vol 9
5. "Essai Sur L’Anatomie Chirurgicale de la Region Iliaque:: Et Description D’un Nouveau Procede: Pour Faire La Ligature Arteres Epigastrique Et Iliaque Externe” J.A. Bogros Imprimerie de E. Duverger. 1827 Paris
- Details

Sagittal section through the clivus of the skull
demonstrating the location of the sphenooccipital
synchondrosis in an infant.
A synchondrosis (plural: synchondroses) is a type of cartilaginous joint characterized by a plate of hyaline cartilage that joins two bones. It is also known as a “primary cartilaginous joint”.
Since a synchondrosis practically has no movement, it is classified as a synarthrosis (plural: synarthroses) an immovable joint. All synchondroses are synarthrotic.
Because of the way bones mature, there are many skeletal synchondroses present while the individual matures, an important group of synchondroses are those of growth plates in long bones at the junction of the epiphysis and the body or shaft of the bone. These disappear when the individual reaches full skeletal maturity.
In the older individual there are a few synchondroses, one of them is found at the joint between the first rib and the sternum, others are found at the costochondral joint, the joint between the ribs and the costal cartilage.
There may be some synchondroses found in areas of skeletal anomalies, like the os acromiale, and tarsal coalitions.
Etymology: The word “synchondrosis” derives from the following medical terminology components: The Greek prefix [σύν] (sýn) meaning “along, with, or plus”, the Greek root term [χόνδρος] from [χόνδρος αρθρώσεων] (chóndros arthróseon), and the suffix [-osis], also Greek, meaning “condition”, “state of” or “many”. The term “synchondrosis” can be loosely interpreted as a “condition with cartilage”.
Sources:
1. “Gray’s Anatomy” Henry Gray, 1918
2. "Tratado de Anatomia Humana" Testut et Latarjet 8th Ed. 1931 Salvat Editores, Spain
3. "Gray's Anatomy" 38th British Ed. Churchill Livingstone 1995
4. "The Origin of Medical Terms" Skinner, HA 1970 Hafner Publishing Co.
Image modified from the original by Henry VanDyke Carter, MD. in the book "Grays's Anatomy" by Henry Gray FRS. Public domain
- Details
UPDATED: One year ago, on Monday January 2nd 2023, Damar Hamlin suffered a cardiac arrest as a consequence of a tackle that impacted his chest. The football player had suffered a Commotio Cordis, a rare but known athletic cardiac injury that was reversed by the medical support teams present at the Cincinnati Football Stadium.
One year later, the University of Cincinnati has published a press release entitled "The Damar Hamlin Effect: Revolutionizing CPR and AED Training Nationwide". Because of this accident, the awareness for training in CardioPulmonary Resuscitation (CPR) and the need and availability of Automated External Defibrillators (AEDs) has increased. His foundation has to-date raised over 9 million dollars!
Following is the original (and updated) post:
I have received several questions regarding this term and its meaning, because of the cardiac arrest suffered on the field by the Buffalo Bills defensive player Damar Hamlin while playing the Cincinnati Bengals on January 2nd, 2023.

01/02/2023 Bengals stadium
For those who were watching the game, close to the end of the first quarter Hamlin blocked another player in what looked like a normal and standard play. Immediately after, Damar Hamlin stood up and immediately collapsed. The video can be seen here. The player was treated on the field and later reports indicated that he had suffered a cardiac arrest and was treated with CPR (manual cardiopulmonary resuscitation), the use of an AED (Automated External Defibrillator) and oxygen. The player was intubated and was considered to be in critical, but stable condition.
The consensus is that Damar Hamlin suffered a ventricular arrhythmia, which allowed the heart to beat erratically, but not be able to pump blood, which is why he had to be defibrillated using the AED.
The cause for this is an uncommon (30 cases per year in the US) but known situation known as Commotio Cordis, a ventricular dysrhythmia caused by a sudden hit to the sternum in a particular location*. It has been seen in baseball and softball players where the pitcher is hit in the sternum by a fast ball coning from first base. Also seen in lacrosse players. In most cases this happens in younger individuals where the four sternabrae that form the body of the sternum have not yet completely ossified, making the sternum and lower costal cartilages quite flexible, being able to “bend in” when hit directly and compress the heart.
As some of you may know, I am a 7th Degree Black Belt in Goju-Ryu Karate. This type of punch to the sternum is one of the many techniques used in advanced Martial Arts. In most cases this punch will slow down an opponent, but it does not cause Commotio Cordis. It is a technique that should only be practiced under very close supervision. In fact, this technique was thought to be legend and was called “the touch of death” in China.

Commotio Cordis at a karate tournament
An example of Commotio Cordis caused by a Karate punch can be see in the following YouTube video. The image in this article shows the instant the chest strike happens at 6 seconds in the video. Look at the hand of the practitioner on the right and the devastating consequence that follows. Please note the similarity of the situation in this video and what happened to Damar Hamlin. There is a lapse of time between the Commotio Cordis cardiac arrest where the athlete gets up or walks followed fainting and unconsciousness. What is distressing is that the young martial artist who suffered this devastating injury died at the tournament. The judges were not aware of the situation, no one felt his pulse, or started life-saving CPR. Because of the content this video is age-restricted and you may have to sign in to view it.
The words are Latin. Commotio means “agitation or commotion”. Cordis means heart. The conditions to cause Commotio Cordis need to be exact, as the heart needs to be in ventricular repolarization, when the heart ventricles are starting to refill with blood. The "window" for a sternal hit to cause Commotio Cordis is very small.
Please, if you do not know how to provide CPR, take a full CPR course or at least attend a short 10 minute training like the one provided by University of Cincinnati Health in their "Take 10 Cincinnati" program.
For additional information please visit StatPearls at https://www.statpearls.com/ArticleLibrary/viewarticle/19761
- Details
How many scientists, physicians, or anatomists have musical pieces written for them? I was so surprised when I found out that there is a musical score entitled “André Vésale” written by Louis-Jean Abadie and published in 1861 in Paris, France. I felt the obligation to research this topic.
There are many people that follow the life and works of Andreas Vesalius, a 16th century anatomist who started the modern scientific approach to human anatomy and medicine. I count myself in this group that includes artists, historians, poets, painters,musicians, medical illustrators, physicians, surgeons, antique collectors, anatomists, etc.
In June 2023, I had the honor of being invited by the University of Antwerp in Belgium to speak at the 2023 Vesalius Triennial Meeting. It was here that I discovered this musical surprise!

Elke Robersscheuten

Theo Dirix
One of the events of this meeting was an afternoon concert entitled “Vesalian landscapes in music, poetry, and photographs” by pianist Elke Robersscheuten, and my friend Theo Dirix, who read the poetry. This was accompanied by slides of Vesalian works, and images of the city of Brussels and the island of Zakynthos, Greece. One of the pieces performed by Elke Robersscheuten was “André Vésale”. You can see Elke perform this piece in a video at the end of this article.
With the help of Theo, I started the process of unraveling the story of this musical piece:

Louis Abadie
The author
Abadie, Louis-Jean (c1814-1858). Louis Abadie was a baritone singer. He started performing in the French provinces as member of an opera troupe. In 1842 he settled in Paris where he wrote numerous chansons and romances which were very popular at the Paris salons at the time. He had success as singer and voice teacher in Paris and in 1848 he released records of his songs, which were well received. I have not been able to find copies of these records.
He went back to traveling and singing, with little success and decided to move to Bordeaux, and then back to Paris where he was unsuccessful trying to find a locale that would present his work to the public. He lived in poverty and in early December 1958 he had a stroke and died at 45 years old, leaving a wife and three children. As a side note to his life, many of his works were dedicated or mentioned by name a woman named Jeanne. His wife's name was Marie Jeanne Toussaint.
Seven years after his death, on May 2, 1867, Les Danseurs de Corde.(The Rope Dancers) , an operetta (comedic opera) in two acts for which he had written the music, was performed at the Théâtre des Folies-Saint-Germain.
The lyrics
The poignant lyrics to this work were written by Louis-Adolphe Turpin de Sansay (1832 – 1891) a prolific French dramatic author, chansonnier, and songwriter. He collaborated with musicians with lyrics for their work. The lyrics for “André Vésale” were written in 1860 and published the following year.
The works of Turpin de Sansay were presented in elite places line the Théâtre des Champs-Élysées, the Théâtre des Bouffes-Parisiens, the Théâtre Beaumarchais, and the Théâtre-Lyrique.
The lyrics for “André Vésale” are based on Vesalius being deported to the Greek island of Zakynthos (known then as Zanthe). We now know this is a legend and not true. Following is the French original and a free translation of this work:
"André Vésale" (French)
Dans un caveau sur ma table de pierre
J'ai de la mort compulsé les secrets.
J'ai de mes mains profané la matière,
Et maintenant j'éprouve des regrets.
Par mon travail si de l'anatomie
J'ai découvert et promulgué la loi:
Si j'ai cherché les sources de la vie,
Pardonnez-moi, mon Dieu, pardonnez-moi!
Ils m'ont banni sur la terre de Zante,
Ils m'ont traité d'impie et d'imposteur;
Et j'ai dû tendre une main suppliante,
Car sur mon front plane le noir malheur!
Mais l'avenir, qui devant moi rayonne,
A ranimé mon courage et ma foi;
Si j'ai rêvé du martyr la couronne,
Pardonnez-moi, mon Dieu, pardonnez-moi!
J'aurais voulu calmer chaque souffrance,
Venir en aide à notre humanité,
Malgré l'exil, cependant, la science
Se répandra dans la postérité!
A mon pays, quoi qu'ingrat, je signale
Mes longs travaux, c'est mon bien, c'est mon droit.
Si j'illustrai le nom d'André Vésale,
Pardonnez-moi, mon Dieu, pardonnez-moi!
"Andreas Vesalius" (English)
In a cellar, on my stone table
I have extracted the secrets of death.
I have desecrated matter with my hands,
And now I feel regret.
By my work of anatomy
I discovered and promulgated the law:
If I sought the sources of life,
Forgive me, my God, forgive me!
They banished me to the land of Zakynthos,
They called me impious and impostor.
And I had to hold out a pleading hand,
For on my forehead hovers black misfortune!
But the future, which shines before me,
Revived my courage and my faith.
If I dreamed of the martyr's crown,
Forgive me, my God, forgive me!
I would have liked to calm each suffering,
Come to the aid of humanity,
Despite the exile, however, science
Will spread to posterity!
To my country, although ungrateful, I point out (that)
My vast work is my property, it is my right.
If I inscribe the name of Andreas Vesalius,
Forgive me, my God, forgive me!
The publisher
Étienne Challiot (1837 – 1866) had his office located at 352-354 Rue St Honoré, in Paris, very close to Place Vendôme, Paris. He published books and music sheets. Some of his publications can be found online.
The printer
Almost nothing is known about the printer of this work. A female printmaker, Madame Dinquel, had her printer shop at 276 Rue Sain Honoré, in Paris, very close to the publisher Étienne Challiot. Today, Sapporo, a Japanese restaurant sits at this address.
The musical piece
Following is a video of pianist Elke Robersscheuten performing "André Vésale" by Luis Abadie.
The original score can be downloaded here. Thanks to IMLSP for preserving this music for posterity. You can click on the image for a larger depiction.
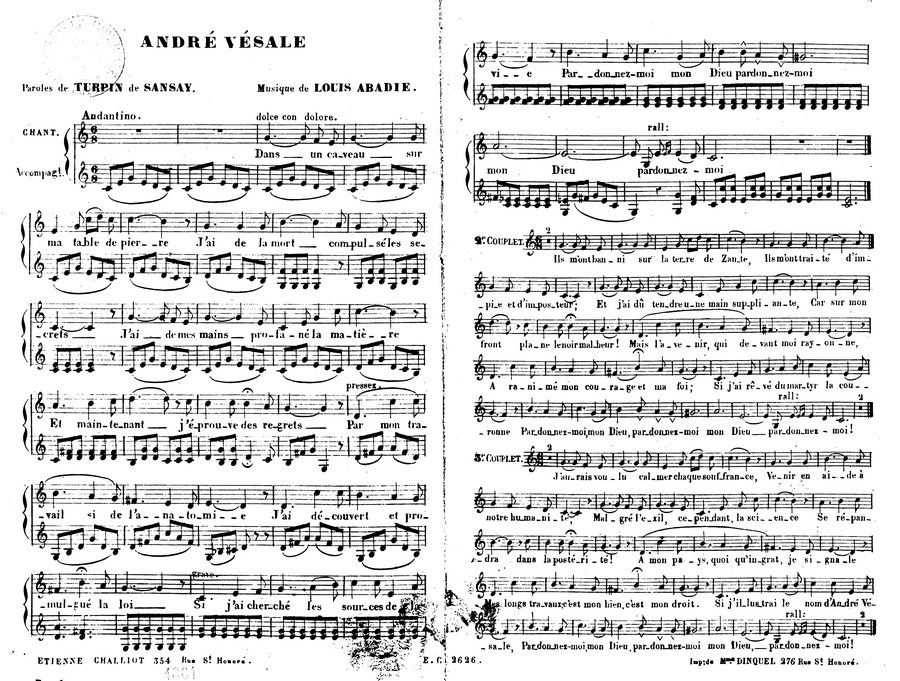
André Vésale sheet music by Luis Abadie. Public Domain
Sources:
1. Biographie universelle des musiciens et bibliographie générale de la musique, Volume 1François-Joseph Fétis Libraire de Firmin-Didot, 1878 Paris
2. Obituary: Courrier de la librairie: journal de la propriété littéraire et artistique pour la France et pour l'étranger. 1858,7/12
3. Necrologie; B. JOUVIN. Théatres (French). Paris: Figaro, 09/12/1858. Article nécrologique dans Le Figaro (Lire en ligne sur Gallica)
4. Obituary: Courrier de la librairie: journal de la propriété littéraire et artistique pour la France et pour l'étranger. 1858,7/12
5. Frédéric Caille, La figure du sauveteur : Naissance du citoyen secoureur en France, 1780-1914, Presses Universitaires de Rennes, 2006, p. 222-224 6.
- Details
Anterior view of the stomach
The term “lesser curvature” refers to the shorter, curved, and concave right-sided border of the stomach. The lesser curvature extends between the esophagogastric junction superiorly and the pylorus inferiorly.
Although generally curved, the lesser curvature presents with a sharp angulation called the incisura angularis or the angular notch.
The lesser curvature is connected to the liver by a double-layered fold of peritoneum called the lesser omentum. The lesser omentum is composed of two regions:
1. The gastrohepatic ligament, the larger component, found between the lesser curvature and the liver. It includes the pylorus.
2. The gastroduodenal ligament, the smaller component, found between the first portion of the duodenum (superior portion, duodenal ampulla) and the liver. The common bile duct is found between the layers of the omentum.
The image shows the lesser curvature with an animated dashed line. The blue arrow points to the incisura angularis.
Sources:
1 "Tratado de Anatomia Humana" Testut et Latarjet 8 Ed. 1931 Salvat Editores, Spain
2. "Anatomy of the Human Body" Henry Gray 1918. Philadelphia: Lea & Febiger
Original pastel image by Dr. E. Miranda