![]()
Medical Terminology Daily (MTD) is a blog sponsored by Clinical Anatomy Associates, Inc. as a service to the medical community. We post anatomical, medical or surgical terms, their meaning and usage, as well as biographical notes on anatomists, surgeons, and researchers through the ages. Be warned that some of the images used depict human anatomical specimens.
You are welcome to submit questions and suggestions using our "Contact Us" form. The information on this blog follows the terms on our "Privacy and Security Statement" and cannot be construed as medical guidance or instructions for treatment.
We have 1274 guests online
")
Marcia Crocker Noyes
(1869 – 1946)
Further to my comment on old books and research that started with an interesting bookplate (Ex-Libris). I continued my research and found that the person in charge of the Osler library bookplate was a fascinating individual that today maybe a ghost in the MedChi library and building in Baltimore... This is certainly an article that can be called "A Moment in History"
Marcia Crocker Noyes was the librarian at The Maryland State Medical Society from 1896 to 1946 and was a founding member of the Medical Library Association.[1][2][3]
Sir William Osler, MD. a famous Johns Hopkins surgeon was a noted bibliophile and had a large personal collection of books on various topics. When he became the President of MedChi in 1896, he was dismayed at the condition of the library and knew that with the right person and some stewardship, it could become a significant collection. Sir William asked his friend, Dr. Bernard Steiner, a physician and President of the Enoch Pratt Free Library in Baltimore for suggestions of a librarian, and Dr. Steiner recommended Marcia Crocker Noyes. A native of New York, and a graduate of Hunter College, Marcia had moved to Baltimore for a lengthy visit with her sister, and took a “temporary” position at the Pratt Library, which turned into three years. Although she had no medical experience or background, she was enthusiastic, and most importantly, she was willing to move into the apartment provided for the librarian, who needed to be available 24 hours a day.
The image in this article is Ms. Noyes on her first year on the job. Marcia developed a book classification system for medical books, based on the Index Medicus, and called it the Classification for Medical Literature. The system uses the alphabet with capital letters for the major divisions of medicine and lower-case ones for the sub-sections. The system was used for many years, but it's now dated and the Faculty's original shelving scheme was never changed. The card catalogs still reflect her classification and many of the cards are written in Marcia's back-slanting handwriting.
Marcia knew enough to ask the Faculty's members about medical questions, terminology and literature. She gradually won over the predominantly male membership and they became her greatest allies; Sir William at the start, and then for nearly 40 years, Dr. John Ruhräh, a wealthy pediatrician with no immediate family of his own. She made a point of attending almost every Faculty function, and in 1904, under guidelines from the American Medical Association, Marcia was made the Faculty Secretary. For much of her first 10 years, she was the Faculty's only full-time employee, only being assisted by Mr. Caution, the Faculty's janitor. Later in life Marcia would say that she hired him because of his name!
Within ten years, the library had outgrown its space, and plans, spearheaded by Marcia and Sir William before his move to Oxford, were made to build a headquarters building, mainly to house the library's growing collection of medical books and journals.
Marcia was instrumental in the design and building of the new headquarters. She travelled to Philadelphia, New York and Boston to look at their medical society buildings, and eventually, the Philadelphia architectural firm, Ellicott & Emmart was selected to design and build the new Faculty building. Every detail of the building held her imprimatur, from the graceful staircase, to the light-filled reading room, and all of the myriad details of the millwork, marble tesserae, and most of all, the four-story cast iron stacks. She was on-site, climbing up unfinished staircases, checking out the progress of the building, which was built in less than one year at a cost of $90,000.
Among the features of the new building was a fourth-floor apartment for her. She referred to it as the "first penthouse in Baltimore" and it had a garden and rooftop terrace. The library collection eventually grew to more than 65,000 volumes from medical and specialty societies around the world. Journals were traded back and forth, and physicians eagerly anticipated the arrival of each new issue. At the same time, Marcia was involved in the Medical Library Association as one of eight founding members. The MLA promotes medical libraries and the exchange of information. One of the earliest mandates of the MLA was the Exchange, a distribution and trade service for those who had duplicates or little-used books in their collections. Initially, the Exchange was run out of the Philadelphia medical society, but in 1900 it was moved to Baltimore and Marcia oversaw it. Several hundred periodicals and journals were received and sent each month, a huge amount of work for a tiny staff. In 1904, the Faculty had run out of room to manage the Exchange, so it was moved to the Medical Society of the Kings County (Brooklyn). But without Marcia's excellent administrative skills, it floundered and in 1908, the MLA asked Marcia to take charge once again.
In 1909, when the new Faculty building opened, there was enough room to run the Exchange and with the help of MLA Treasurer, noted bibliophile and close friend, Dr. John Ruhräh, it once again became successful. Additionally, Marcia and Dr. Ruhräh combined forces to revive the MLA's bulletin, which had all but ceased publication in 1908, taking the Exchange with it. This duo maintained editorial control from 1911 until 1926. In 1934, around the time of Dr. Ruhräh's death, Marcia became the first “unmedicated” professional to head the MLA. During her tenure, the MLA incorporated, the first seal was adopted, and the annual meeting was held in Baltimore. Marcia wanted to write the history of the MLA once she retired from full-time work at the Faculty, but her health was beginning to fail. She had back problems and had suffered a serious burn on her shoulder as a young woman, possibly from her time running a summer camp, Camp Seyon, for young ladies in the Adirondack Mountains. In 1946, a celebration was planned to honor Marcia's 50 years at the Faculty. But she was adamant that the physicians wait until November, the actual date of her 50 years. However, they knew she was gravely ill, and might not make it until then, so a huge party was held in April. More than 250 physicians attended the celebration, but the ones she was closest to in the early years, were long gone. She was presented with a suitcase, a sum of money to use for travelling, and her favorite painting of Dr. John Philip Smith, a founder of the Medical College in Winchester, Virginia. It was painted by Edward Caledon Smith, a Virginia painter who had been a student of the painter Thomas Sully.[4] She adored this painting and vowed, jokingly, to take it with her wherever she went.
The painting was not to stay with her for very long, for she died in November 1946, and left it to the Faculty in her will. Her funeral was held in the Faculty's Osler Hall, named for her dear friend. More than 60 physicians served as her pallbearers, and she was buried at Baltimore's Green Mount Cemetery. In 1948, the MLA decided to establish an award in the name of Marcia Crocker Noyes. It was for outstanding achievement in medical library field and was to be awarded every two years, or when a truly worthy candidate was submitted. In 2014, the Faculty began giving a bouquet of flowers to the winner of the award in Marcia's name, and in honor of her work. Much evidence exists for this tradition, as we know that the physicians, especially Drs. Osler and Ruhräh, frequently gave her bouquets of flowers. Marcia also cultivated flower gardens at the Faculty and decorated the rooms with her work.
Today, the MedChi building is open for tours and if the rumors are to be believed Ms. Marcia Crocker Noyes is still at work in her beloved library as the "resident ghost" [1][5]

NOTE: This article has been modified from the original Wikipedia article on Marcia Crocker Noyes. The article itself is well-written with interesting images of the subject. I would encourage you to visit it. The second insert is from book 00736 in my personal library and shows in pencil, the incredibly small handwriting of Marsha C. Noyes.
Sources:
1. "Marcia, Marcia, Marcia" MedChi Archives blog.
2. "Marcia C. Noyes, Medical Librarian" (PDF). Bulletin of the Medical Library Association. 35 (1): 108–109. 1947. PMC 194645
3. Smith, Bernie Todd (1974). "Marcia Crocker Noyes, Medical Librarian: The Shaping of a Career" (PDF). Bulletin of the Medical Library Association. 62 (3): 314–324. PMC 198800Freely accessible. PMID 4619344.
4. Edward Caledon BRUCE (1825-1901)"
5. Behind the scenes tour MedChiBuilding
"Clinical Anatomy Associates, Inc., and the contributors of "Medical Terminology Daily" wish to thank all individuals who donate their bodies and tissues for the advancement of education and research”.
Click here for more information
- Details
Anterior view of the stomach
The term "incisura" is Latin, derived from the verb [incidere]* meaning "to cut" or [incisura]” meaning a "notch" or indentation in a structure, suggesting a distinctive incision, or cut. The second component, "angularis," is also Latin, derived from "angulus," which translates to "angle." The term "incisura angularis" can be translated as the "angular notch", a term that is also use for this gastric anatomical landmark.
The incisura angularis is a notch located along the lesser curvature of the stomach. Externally, it marks the transition between the body (corpus) and antrum of the stomach, an abdominal viscus. It is related to the gastrohepatic portion of the lesser omentum superolaterally. It should be mentioned that the lesser curvature vascular arcade runs within the lesser omentum, closely related to the gastric lesser curvature.
Found approximately midway between the esophagogastric junction and the pylorus, this external anatomical feature is easily identifiable internally during gastric endoscopy.
Structurally, the incisura angularis is formed by a fold of mucous membrane on the inner surface of the stomach, creating a small recess along the lesser curvature.
The stomach, although it has the same layers as the rest of the GI tract, presents an extra muscular layer in the area of the lesser curvature, which renders this area less distensible forming a muscular channel called the magenstrasse.
The mucosa layer is the deepest of the stomach layer. Within it, three areas of gastric mucosa are usually described: pyloric, transitional, and fundic. The incisura angularis corresponds mostly to the transitional zone. When there are mucosal changes that shown an invasion of another type of mucosa, it can mean preneoplastic changes. For this reason, the incisura angularis is an area that, when biopsied, can show early cancerous changes, as well as muscular atrophy, intestinal metaplasia, and dysplasia.
Preservation of the anatomy of the incisura angularis is critical during a sleeve gastrectomy, the most common bariatric procedure worldwide. The objective of a sleeve gastrectomy is to reduce the size of the stomach by placing a curved staple line along the left border of the magenstrasse, a lesser known gastric anatomy term.
Because of the location of the incisura angularis, improper placement of a straight gastric stapler could cause stenosis or stricture at this level. Another potential postoperative problem in this procedure is gastroesophageal reflux disease (GERD) where some authors have proposed an omentopexy as a way to modify the angle of the incisura angularis.
Sources:
1. "The Origin of Medical Terms" Skinner, HA 1970 Hafner Publishing Co.
2. "Medical Meanings - A Glossary of Word Origins" Haubrich, WD. ACP Philadelphia
3 "Tratado de Anatomia Humana" Testut et Latarjet 8 Ed. 1931 Salvat Editores, Spain
4. “The Rarely Sampled Incisura Angularis Is Useful for the Detection of Gastric Preneoplastic Lesions” Singhal, A. , Saboorian, H. , Turner, K. , Rugge, M. & Genta, R. (2023). The American Journal of Gastroenterology, 118 (10S), S1407-S1407.
5. “Incisura angularis belongs to fundic or transitional gland regions in Helicobacter pylori-naive normal stomach: Sub-analysis of the prospective multi-center study” Nakajima, S at al Digestive Endoscopy 2021; 33: 125–132
6. “Increasing the angle at the incisura angularis using omentopexy reduces/prevents GERD symptoms five years after laparoscopic sleeve gastrectomy?” Presidential Grand Rounds. Surgery for Obesity and Related Diseases, Volume 18, Issue 8, Supplement, 2022
7. “Gastric POEM to treat incisura angularis torsion after sleeve gastrectomy” Baptista, A; Davila, M; Guzman, M. Endoscopy 2019; 51(04)
8. “Obstruction after Sleeve Gastrectomy, Prevalence, and Interventions: a Cohort Study of 9,726 Patients with Data from the SOReg” Sillen, L; Andersson, E, Edholm, D. OBES SURG 31, 4701–4707 (2021)
Note: Google Translate includes the symbol (?). Clicking on it will allow you to hear the pronunciation of the word.
- Details
[UPDATED] This is a medical term derived from the Latin [incisus] or [incisura], meaning "to cut". The Greek word [Τομή] (tomí) from which the suffixes [-otome], or [-otomy] derive, have a similar meaning.
The root term is [-cis-] and uses of this term include:
- Incision : "To cut in" • Incisive: Something that "cuts in"
- Incisor: Refers to a type of tooth that has a "cutting in" action
- Excision: The prefix [ex-] means "out" or "outside". To cut out, or to extirpate. See the meaning of the suffix [-ectomy] here
- Circumcision: The prefix [circum-] means "around", or "in a circle". To cut around (in a circle)
Note: Google Translate includes an icon that will allow you to hear the pronunciation of the word
- Details
- Written by: Efrain A. Miranda, Ph.D.
Lateral view - Human embryo about
eight and a half weeks old
(UPDATED) The term [ventral] arises from the Latin word [venter] and the root term [ventr-] meaning "belly" or "sac". The adjective [ventral] means "towards the front" , or "towards the belly side of the body". The term ventral therefore means "abdomen".
Many use the term [ventral] synonymously with "anterior"; although this is technically correct, the proper term to use when referring to the patient in the anatomical position should be "anterior". In embryology, since the embryo is curved, most of the anterior aspect of the embryo looks towards the abdomen, ergo ventral.
A ventral hernia is any herniation that occurs in the anterior aspect of the abdomen, including Spigelian hernias, omphaloceles, etc.
Other terms that arise from the same root term are [ventricle], meaning "little belly", or "little sac", and [ventricular], meaning "pertaining to a ventricle".
Note: A comment from my friend Dr. Elizabeth Murray:
"My understanding of "anterior" means "in the direction of movement" for any given organism (and "posterior" means opposite the direction of movement for an organism). Thus, ventral does not ever change for any creature (vertebrate or even invertebrate), as it refers to a body part/surface. But when considering two-legged and four-legged (or finned) creatures, you see the differences: Ventral = anterior in us, but in a dog or fish ventral = inferior.
Ventral/dorsal refer to belly/back in any organism, and cranial/caudal refer to head-end and tail-end in any organism -- those four terms refer to body parts. However, anterior/posterior refer to the way an organism moves in space, and superior/inferior refer to an organism's relationship to the earth/pull of gravity."
An interesting side note: The word [ventriloquist] arises from the root term [-ventri-] from the Latin [venter] and the suffix [-loquist], from the Latin [loquos] and [locutus], meaning "to speak", or "someone who speaks". The term [ventriloquist] means then "someone who speaks from the abdomen (or stomach)". We now know that this is not so, but that is what most people think a ventriloquist does!
Sources:
1 "Tratado de Anatomia Humana" Testut et Latarjet 8 Ed. 1931 Salvat Editores, Spain
2. "Anatomy of the Human Body" Henry Gray 1918. Philadelphia: Lea & Febiger
Image modified by CAA, Inc. Original image by Henry Vandyke Carter, MD., courtesy of bartleby.com
- Details
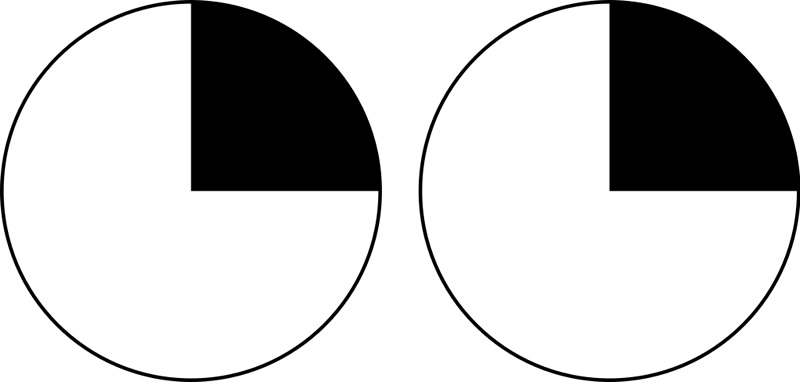
Right homonymous superior quadrantanopia
[Quadrant]-[an-[opia ] The root “quadrant” is based on the Latin "Quadri" meaning "four" and “Quarto”, meaning one fourth. The suffix anopia is composite: “an” meaning “without or absence of”; and opia (or “opsia”) relate to vision, based on the Greek word “οπτασία” (optasía) meaning “sight”. Literally, the term quadrantanopia (or quadrantanopsia) means “absence of sight in a quadrant”.
It can be associated with a lesion of an optic radiation of the internal capsule. While quadrantanopia can be caused by lesions in the temporal and parietal lobes of the brain, it is most commonly associated with lesions in the occipital lobe.
What is interesting are the terms “homonymous” and “heteronymous” used to describe variants of quadrantanopia. Each eye has four quadrants and two visual fields, right and left. A homonymous quadrantanopia means that the patient has lost the vision of a quadrant in the same field in each eye (right-right or left-left), heteronymous means that the patient has lost the vision of a quadrant in the opposite field of each eye (right-left or left-right).
The fact is that the term homonymous means “same name” not same side, and the word heteronymous means “different name”, from the Greek “όνομα” “nym” meaning name. For further confirmation, try finding the meaning of synonym, antonym, acronym, patronymic, etc.
Sources:
1. "The Origin of Medical Terms" Skinner, HA 1970 Hafner Publishing Co.
2. "Medical Meanings - A Glossary of Word Origins" Haubrich, WD. ACP Philadelphia
3. "Dorlands's Illustrated Medical Dictionary" 26th Ed. W.B. Saunders 1994
Note: Google Translate includes an icon that will allow you to hear the pronunciation of the word
Image courtesy of Mudsk, CC0, via Wikimedia Commons.
- Details
- Written by: Efrain A. Miranda, Ph.D.
- Hits: 2209
I had the honor of being invited to participate in the 53rd Annual Chilean Meeting of Anatomy (XLIII Congreso Chileno de Anatomía) which was held in conjunction with the 1st Latin American Congress of Clinical Morphology (Primer Congreso Latinoamericano de Morfología Clínica). Along with these meetings were two symposia: The First Joint Symposium of Chilean/Korean Anatomists and the First Joint Chilean - IFAA-FIPAE Symposium (International Federation of Associations of Anatomists - Federative International Program for Anatomy Education).

Universidad de Los Andes, Chile
This meeting was held on November 11- 14, 2023 and was hosted by the University of Los Andes (Universidad de Los Andes), a Chilean institution of private higher education that offers careers and postgraduate programs in different areas of knowledge including Education, Engineering, Nursing, Obstetrics, Medicine, Psychology, Law. etc. Their campus is located on the slopes of the beautiful Andes mountains overlooking the city of Santiago, Chile.
The image shows the Main Library of the University, where the meeting was held.
On November 9 and 10, the days leading to the meeting, there were six Postgraduate Courses, from anatomy to radiology and surgical reconstruction. There were two that I would like to highlight. The first one was a workshop "Mastering Anatomical Radiology with IMAIOS", where one of the instructors was my good friend Dr. Cristian Uribe, who was one of the Meeting organizers. Dr. Uribe is one of the contributors to Medical Terminology Daily.
The second one was a "Workshop on Art & Science: A Theoretical-Practical Course on Anatomical Illustration". This course was directed by my good friend, Dr. Carlos Machado, world-renown medical illustrator, physician, and anatomist, editor of Netter's Atlas of Anatomy. Along with him two professors, Drs. Daniel Casanova and Valentina Cerda.

Nov. 11, 2023 Meeting opening
The Meeting was officially opened by Dr. Juan Carlos Lopez, Director of the Morphology Department of the Los Andes University. This was followed by a presentation on "The Role of the Placenta on the Modulation of Human Potential" by Dr. Sebastian Illanes. On the picture, from left to right, Dr. Jens Wasche (Germany), Dra. Valentina Cerda (Chile), Dr. Carlos Machado (Brazil/USA), me (Chile/USA), and Dr. Andres Riveros Valdes (Chile), a good friend and anatomist. Dr. Riveros is the President of the LatinAmerican Meeting on Clinical Morphology.
There were so many great presentations in this meeting! I think the attendees will agree with me that the conference by Dr. Carlos Machado on "The Art of Learning and Teaching Anatomy with Art" was one of the highlights of the Meeting. In his presentation Dr. Machado shared some of his early drawings and his career in Medicine and Medical Illustration, how he has used art to show patient pathology, and most important, the work and dedication that is required when developing a single image that will later become part of the Anatomy Atlases with which he collaborates.
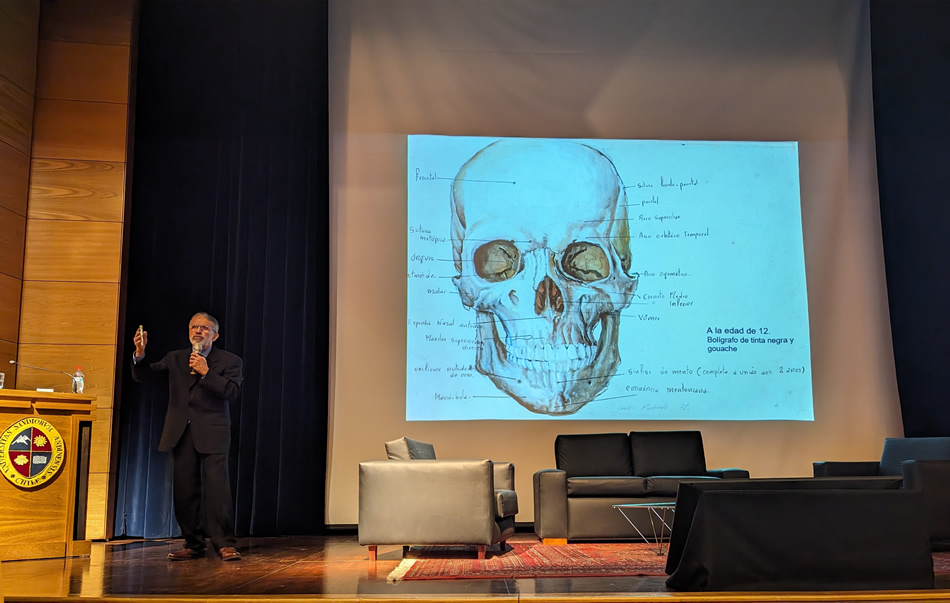
Dr. Carlos Machado
The image above shows Dr. Machado during his presentation. On the screen an anatomical image he drew when he was 12 year old!.

Dr. Carlos Machado

Dr. Cristian Uribe

Poster presentations during a coffee break
The meeting was also geared toward morphology students of different careers including Veterinary, Nursing, Dental School, and Medicine. The students presented their research posters during the coffee breaks. There were very high-quality and in-depth research, including the first osteology atlas of the Chilean flamingo (Phoenicopterus chilensis). I had interesting discussions on Latin terminology with these students.
There were extremely interesting topics throughout the week, including liver anatomy and liver transplant, ethics, philosophy, body donation, etc.
My presentation was based on the conference I delivered in May 2023 at the University of Antwerp, Belgium. Since the Belgium conference was delivered to a group of Andreas Vesalius experts, this one included much more information on Andreas Vesalius, his work, and additional information on printing techniques circa 1550.
Dr. Miranda during his presentation at the
XLIII Anatomy Meeting in Chile
The presentation added information on the history of the woodblocks used to print the 1543 Fabrica, the 1555 Fabrica, as well as other books that include the 1925 "The Iconography of Andreas Vesalius" by M.H. Spellman, and the 1934 Icones Anatomicæ.
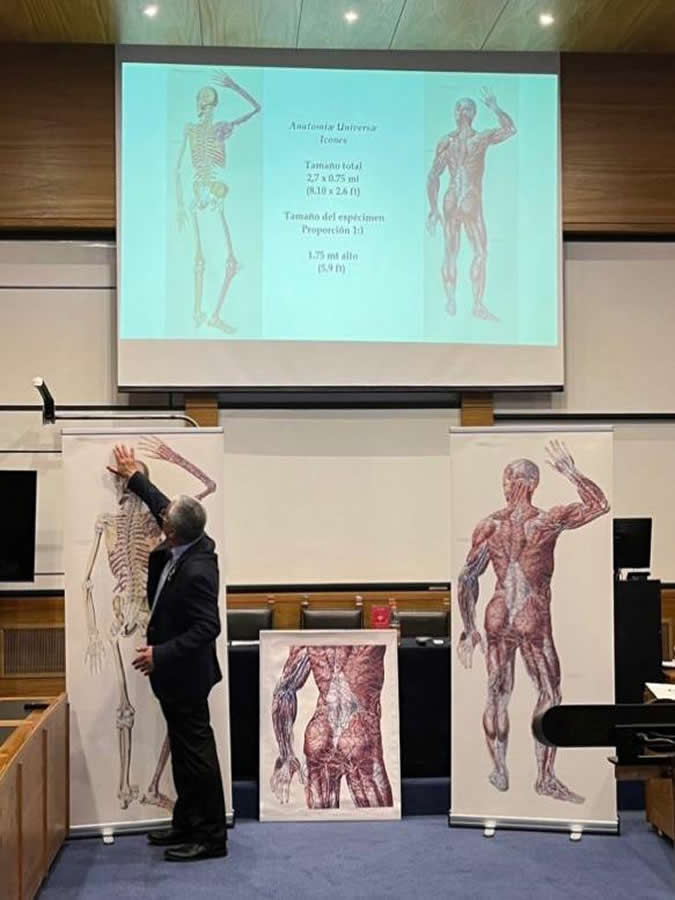
The included picture was taken towards the end of my presentation where with the help of Dr. Uribe we unveiled Giovanni Paolo Mascagni's (1755-1815) work. At the center is a life-size copy of one of the pages of his book "Anatomiæ Universæ Icones", published in 9 installments between 1823 and 1832. It is important to note that each page of this book was hand-colored by Antonio Serantoni (1780-1837), thus the time it took to print and publish this book.
Mascagni's book, the largest book ever printed, shows in separate pages one third of a larger, life-size individual. Because of the rarity and value of this magnificent work, it cannot be cut and pasted.There are 16 know copies of Mascagni's anatomical opus magnus in the world, one of them at the University of Cincinnati, Ohio. USA.
With the help of Mr. Gino Pasi curator of the Henry Winkler Center for the History of the Health Professions, and the help of Mrs. Samantha Scheck, graphic designer, we measured and scanned some pages of the "Anatomiæ Universæ Icones", cleaned the background (no changes were done to the image itself) and pasted them digitally. The result is a life-size male 5.9 ft tall (1,75 mt). The images are incredible, and having traveled back and forth to Belgium and Chile, they are now part of my personal library.
Once again, my thanks to my old and new friends for making my stay so interesting, both personally and professionally. My thanks to the organizers of these meetings and symposia:
Dr. Juan Carlos López Navarro
President XLIII Chilean Anatomy Meeting
Director Morphology Department - Universidad de Los Andes
Dr. Andrés Riveros Valdés
President I Latin American Clinical Morphology Meeting
Professor - Universidad San Sebastián
Dra. Viviana Toro Ibacache
President Scientific Committee
Professor - Universidad de Chile
Dr. Emilio Farfán Cabello
President Chilean Anatomy Society
Professor - Pontificia Universidad Católica de Chile
- Details
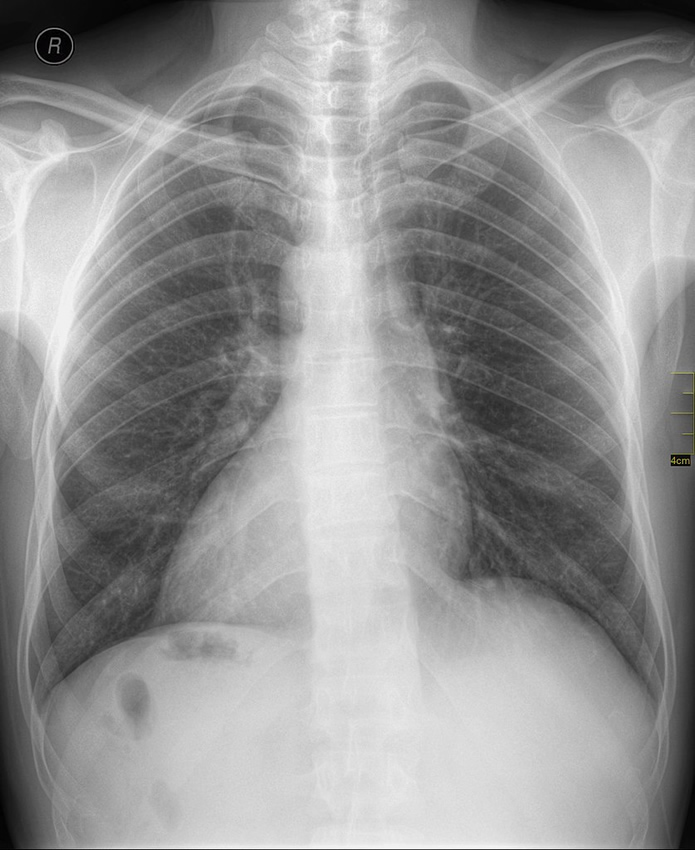
Chest X-Ray - dextrocardia
Normally, the heart is a midline structure found just posterior to the sternum where 35-40% of the heart mass in the right side of the thorax (chest), and the rest (60-65%) is in the left side of the thorax. In this normal condition the apex of the heart faces slightly inferior and to the left. In fact, there are many books and websites that state (wrongly) that the heart is normally in the “left side of the chest”.
If the above mentioned situation is reversed, we are in the presence of dextrocardia, that is, the heart is still in the midline, but most of the mass of the heart is in the right side of the thorax, and the apex points inferiorly and to the right.
The word dextrocardia is a derivate of the Latin [dexter], meaning “right”, and the Greek term [kardia], meaning “heart”. The word dextrocardia literally means “right-sided heart”.
Dextrocardia is a congenital condition, can be completely asymptomatic and present as an isolated condition. It can also be part of a complex genetic condition called “situs inversus” where the whole body is a mirror image of itself and all organs, including the heart are mirrored. A complete situs inversus is rare, but when present it usually does not cause problems.
The problems start when only part of the body and organs are reversed and others are not, causing an incredible number of potential anatomical variations and associated problems.
The prevalence of dextrocardia is about 1 in 12,00 pregnancies. The reported incidence is about 0.22%. Depending on the situation, dextrocardia can present with additional cardiac congenital disorders.
Sources:
1. “Dextrocardia: an incidental finding” Yusuf SW, Durand JB, Lenihan DJ, Swafford J. Tex Heart Inst J 2009;36(4):358-9.
2. Garg N, Agarwal BL, Modi N, Radhakrishnan S, Sinha N. Dextrocardia: an analysis of cardiac structures in 125 patients. Int J Cardiol 2003;88(2–3):143–56
3. Bernasconi A, Azancot A, Simpson JM, Jones A, Sharland GK. Fetal dextrocardia: diagnosis and outcome in two tertiary centres. Heart 2005;91(12):1590–4.