|
The [ureters] are two long, thin, bilateral muscular tubes that extend from the pelvis of the ipsilateral kidney to the posteroinferior aspect of the urinary bladder. The ureters are retroperitoneal structures and their function is the transport of urine between the kidney and the urinary bladder.
The word arises from the Greek [ουρητήρ], meaning "urinary duct". The term was originally used to denote both the urethra (in its singular form) and the ureters (in its plural form). Because of the problems using the term, the word [urethra] was created.
The ureter is composed of three layers: a mucosa, a thick muscular layer, and an adventitia. The muscular layer is itself composed of an deep longitudinal layer and a superficial circular layer formed by spiral smooth muscle fibers. In the distal portion of the ureter there is a third layer added to the ones mentioned, a thick longitudinal layer that extends into the walls of the urinary bladder. Since the ureter is a retroperitoneal organ, in the areas where the ureter is in contact with the parietal peritoneum, it can be said that the ureter presents with a fourth layer. The muscular construction of the ureters in layers allows for peristalsis that helps the flow of urine.
|
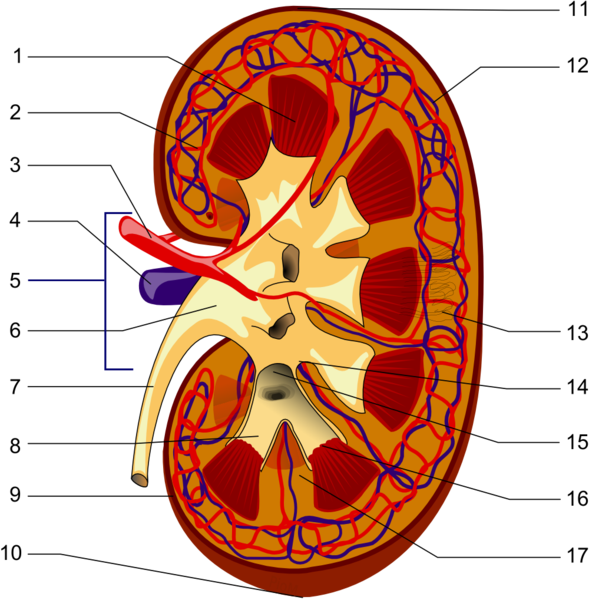
Longitudinal section of a kidney. 1-Renal pyramid, 3-Renal artery, 4-Renal vein, 5-Renal hilum, 6-Renal pelvis, 7- Ureter, 8-Minor calyx, 9-Renal capsule, 14-Minor calyx, 15- Major calyx, 16-Renal papilla, 17-Renal column .
|
| In the female the pelvic ureter passes just inferior to the uterine artery, as situation that surgeons refer to as "water under the bridge". Proper identification of the ureter is critical to avoid damage to this structure during a total hysterectomy. Surgeons will use the peristaltic movement of the ureter to identify it.
In its trajectory the ureters descend anterior to the psoas major muscle, pass over the pelvic brim, just anterior to the origin of the internal iliac artery, then hug the lateral pelvic wall and enter the urinary bladder from a posteroinferior aspect. As it descends the ureters receive blood supply from different arteries: renal arteries, gonadal (testicular or ovarian) arteries, aorta, common iliac arteries, and the inferior vesical arteries. The ureters also receive sympathetic and parasympathetic innervation from the autonomic nervous system renal plexus.
Sources
1. "Gray's Anatomy"38th British Ed. Churchill Livingstone 1995
2. "Tratado de Anatomia Humana" Testut et Latarjet 8 Ed. 1931 Salvat Editores, Spain
3. "The origin of Medical Terms" Skinner, AH, 1970
4. "Histology; a Text and Atlas" Ross MH 3rd Ed. Williams and Wilkins 1995
Images courtesy of Wikipedia
|